August 19, 2021 | Jessica Zeff
3 Minute Read
Summary of 2022 Hospice Payment Rate Final Rule
New rules and policy changes are certainly keeping the hospice sector busy. First, the moratorium on hospice sequestration and now the 2022 Hospice Payment Rate Final Rule!
Your compliance eyes and ears here at Net Health have had their noses to the ground (or, rather, nose to the regulatory grindstone) and we’ve put together a detailed summary of key things to know about sequestration and the 2022 final rule so you don’t have to!
Moratorium on Hospice Sequestration
- Sequestration put into effect as part of the Budget Control Act of 2011, involving a series of spending cuts aimed at reducing our national deficit
- Cut included a 2% sequestration for hospice agencies
- Bill signed into law in April: sequestration reduction will not be applied to Medicare payments, at least, through December 31, 2021.
- Recognizes how hard the sector has been affected by the COVID-19 PHE
2022 Hospice Payment Rate Final Rule: Medicare Hospice Payment Policies
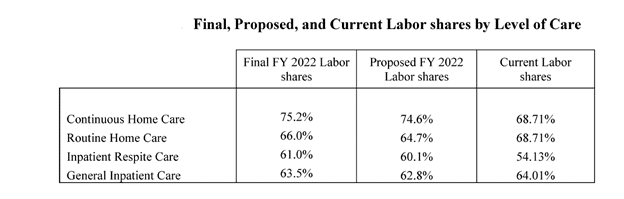
CMS has finalized rebasing the labor shares for all four levels of care: routine home care (66%), continuous home care (75.2%), inpatient respite care (61%), and general inpatient care (63.5%) based on the compensation cost weights for each level of care from the 2018 Medicare cost report data for freestanding hospices.
Routine Annual Rate Setting Changes
CMS finalized a 2.0 percent increase ($480 million) in payments to hospices for FY 2022. This represents a 2.7 percent market basket percentage increase reduced by a 0.7 percentage point productivity adjustment.
CMS also confirmed it will apply a 2% reduction to the annual hospice payment update percentage increase for hospices that fail to meet quality reporting requirements.
FY 2022 hospice payment updates also includes an update to the statutory aggregate cap amount. The cap amount for FY 2022 is $31,297.61.
Hospice Wage Index Updates
Hospice Wage Index updates are as follows:
The final hospice wage index applicable for FY 2022 (October 1, 2021-September 30, 2022) can be found HERE
Hospice Conditions of Participation (CoPs)
CMS has finalized changes to the hospice CoPs regarding hospice aide competency evaluation standards. If there is a specific area of concern that is verified during the on-site visit, the hospice must conduct, and the hospice aide must complete a competency evaluation of the deficient skill. This change will allow hospices to focus on deficiencies and skills instead of all areas in the competency evaluation.
CMS has also approved the use of the pseudo-patient for the hospice aide competency training. Previously, competency training had to occur with real patients. A Pseudo-patient can be a person trained to participate in a role-play situation, or a computer-based mannequin device. A pseudo-patient must be capable of responding to and interacting with the hospice aide trainee and must demonstrate the general characteristics of the primary patient population served by the hospice in key areas such as age, frailty, functional status, cognitive status, and care goals.
Hospice Quality Reporting Program (HQRP)
CMS has confirmed that the HQRP will contain four quality measures that capture care across the hospice stay:
- Consumer Assessment of Healthcare Providers and Systems (CAHPS) Hospice Survey Measure (NQF#2651)
CAHPS is a patient experience survey which is used in Medicare’s STAR Ratings program. CAHPS information for hospices will now be reported on Care Compare to make it easier for patients to compare services between hospices. - HIS Comprehensive Assessment Measure (NQF#3235)
The rule confirms that the HIS Hospice Comprehensive Assessment Measure (NQF# 3235) will replace the following seven HIS process measures beginning FY 2022:
- NQF #1617 Patients Treated with an Opioid who are Given a Bowel Regimen
- NQF #1634 Pain Screening
- NQF #1637 Pain Assessment
- NQF #1638 Dyspnea Treatment
- NQF #1639 Dyspnea Screening
- NQF #1641 Treatment Preferences
- NQF #1647 Beliefs/Values Addressed
3. Hospice Visits in the Lasts Days of Life (HVLDL) – NEW Claims-based Measure
HVLDL assesses hospice staff visits to patients at the end of life and is constructed from Medicare hospice claims records. Specifically, it indicates the provider’s proportion of patients who have received in-person visits from a nurse or medical social workers at least two out of the final three days of the patient’s life.
HVLDL replaces the HIS Hospice Visits When Death is Imminent (HVWDII) quality measure and Section O (service utilization) of the HIS. It will not impose any new requirements for data collection. Instead, this measure will utilize eight quarters of claims data. CMS may start publicly reporting HVLDL as soon as May 2022 but not before then.
4. Hospice Care Index (HCI) Measure – NEW Claims-based Measure
HCI is a single measure compromising ten indicators calculated from Medicare claims data. The index design of the HCI monitors all 10 indicators at the same time. The data source for this measure will be Medicare claims data that are already collected and submitted to CMS. CMS intends to start reporting this measure using existing data items as early as May 2022.
Detailed HCI Indicators are as follows:
(1) Continuous Home Care (CHC) or General Inpatient (GIP) Provided
- Numerator: The total number of CHC or GIP services days provided by the hospice within a reporting period.
- Denominator: The total number of hospice service days provided by the hospice at any level of care within a reporting period.
- Index Earned Point Criterion: Hospices earn a point towards the HCI if they provide at least one CHC or GIP service day within a reporting period.
(2) Gaps in Skilled Nursing Visits
- Numerator: The number of elections with the hospice where the patient experiences at least one gap between nursing visits exceeding 7 days, excluding hospice elections where the patient elected hospice for less than 30 days within a reporting period.
- Denominator: The total number of elections with the hospice, excluding hospice elections where the patient elected hospice for less than 30 days within a reporting period.
- Index Earned Point Criterion: Hospices earn a point towards the HCI if their individual hospice score for gaps in skilled nursing visits greater than 7 days falls below the 90th percentile ranking among hospices nationally.
(3) Early Live Discharges
- Numerator: The total number of live discharges from the hospice occurring within the first 7 days of hospice within a reporting period.
- Denominator: The total number of all live discharge from the hospice within a reporting period.
- Index Earned Point Criterion: Hospices earn a point towards the HCI if their individual percentage of live discharges on or before the seventh day of hospice falls below the 90th percentile ranking
(4) Late Live Discharges
- Numerator: The total number of live discharges from the hospice occurring on or after 180 days of enrollment in hospice within a reporting period.
- Denominator: The total number of all live discharge from the hospice within a reporting period.
- Index Earned Point Criterion: Hospices earn a point towards the HCI if their individual hospice score for live discharges on or after the 180th day of hospice falls below the 90th percentile ranking among hospices nationally.
(5) Burdensome Transitions (Type 1)—Live Discharges From Hospice Followed by Hospitalization and Subsequent Hospice Readmission
- Numerator: The total number of live discharges from the hospice followed by hospital admission within 2 days, then hospice readmission within 2 days of hospital discharge within a reporting period.
- Denominator: The total number of all live discharge from the hospice within a reporting period.
- Index Earned Point Criterion: Hospices earn a point towards the HCI if their individual hospice score for Type 1 burdensome transitions falls below the 90th percentile ranking among hospices nationally.
(6) Burdensome Transitions (Type 2)—Live Discharges From Hospice Followed by Hospitalization With the Patient Dying in the Hospital
- Numerator: The total number of live discharges from the hospice followed by hospitalization within 2 days of live discharge with death in the hospital within a reporting year.
- Denominator: The total number of all live discharges from the hospice within a reporting year.
- Index Earned Point Criterion: Hospices earn a point towards the HCI if their individual hospice score for Type 2 burdensome transitions falls below the 90th percentile ranking among hospices nationally.
(7) Per-Beneficiary Medicare Spending
- Numerator: Total Medicare hospice payments received by a hospice within a reporting period.
- Denominator: Total number of beneficiaries electing hospice with the hospice within a reporting period.
- Index Earned Point Criterion: Hospices earn a point towards the HCI if their average Medicare spending per beneficiary falls below the 90th percentile ranking among hospices nationally.
(8) Skilled Nursing Care Minutes per Routine Home Care (RHC) Day
- Numerator: Total skilled nursing minutes provided by a hospice on all RHC service days within a reporting period.
- Denominator: The total number of RHC days provided by a hospice within a reporting period.
- Index Earned Point Criterion: Hospices earn a point towards the HCI if their individual hospice score for Skilled Nursing Minutes per RHC day falls above the 10th percentile ranking among hospices nationally.
(9) Skilled Nursing Minutes on Weekends
- Numerator: Total sum of minutes provided by the hospice during skilled nursing visits during RHC services days occurring on Saturdays or Sunday within a reporting period.
- Denominator: Total skilled nursing minutes provided by the hospice during RHC service days within a reporting period.
- Index Earned Point Criterion: Hospices earn a point towards the HCI if their individual hospice score for percentage of skilled nursing minutes provided during the weekend is above the 10th percentile ranking among hospices nationally.
(10) Visits Near Death
- Numerator: The number of decedent beneficiaries receiving a visit by a skilled nurse or social worker for the hospice in the last 3 days of the beneficiary’s life within a reporting period.
- Denominator: The number of beneficiaries with at least 1 day of hospice during the last 3 days of life within a reporting period.
- Index Earned Point Criterion: Hospices earn a point towards the HCI if their individual hospice score for percentage of decedents receiving a visit by a skilled nurse or social worker in the last 3 days of life falls above the 10th percentile ranking among hospices nationally.
Hospice Outcomes & Patient Evaluation (HOPE)
The Hospice Outcomes & Patient Evaluation (HOPE) is the new standardized patient assessment tool being developed by CMS. CMS is anticipating that HOPE will replace the Hospice Item Set (HIS), the current patient level data collection tool. Currently, CMS has no deadline or plan for implementation as they are still field testing the new tool.
Text Changes for the Hospice Election Statement Addendum
This final rule clarifies several ambiguities in the original language which defined addendum* requirements. The clarifications are in italics.
- If patient requests addendum in the first five days of care, providers have five calendar days to deliver the addendum to the patient. If patient requests the addendum any time after the first five days of care, hospice now has three calendar days to send it to the patient.
- Language is changed from 72 hours to three calendar days – the change in language provides hospices with an extended timeframe
- 3- or 5-day requirement is tied to when the provider furnishes the addendum, not when it is signed, so important to document when the addendum is furnished.
- Provider must discuss the addendum with the patient at the time of election and document this – even if the patient does not ask for the addendum.
- Medicare payment is contingent on a hospice having a signed addendum.
- If a patient refuses to sign the addendum, the provider must document on the addendum itself, not in the medical record, why the patient refused to sign.
- Non hospice providers requesting the addendum are not required to sign it
- If the patient dies, revokes election, or is discharged within the required timeframe (3 or 5 days after a request, depending upon when such request was made), but the hospice has not yet furnished the addendum, the hospice is not required to furnish the addendum to receive payment for this activity.
Fast Healthcare Interoperability Resources (FHIR) in Support of the Hospice QRP
CMS is asking for comments on advancing to digital quality measurement and the use of FHIR in reporting hospice measure data.
Home Health Quality Reporting Program
CMS is proposing to use three quarters rather than four quarters of data for the January 2022 refresh affecting OASIS-based data.
For certain claims-based measures, CMS is also proposing to use three quarters of data for refreshes between January 2022 and July 2024.
Public reporting with refreshed data to begin January 2022.
Health Equity Gaps
CMS is looking to stratify quality measure data by race and ethnicity with the intention of identifying quality care gaps in relation to specific at-risk groups, supporting health equity strategies, and encouraging improvement in health outcomes.
References and Resources:
Model Hospice Election Statement Addendum